{kind=link}
{kind=link}
Interesting Cases
- Root Canal Therapy-Maxillary 1st Molars
- Retreatment Root Canal Therapy
- Apicoectomy (Surgical Root Canal Treatment)
- Clinical Crown Lengthening
- Intravenous Sedation (IV Sedation)
- Block Bone Grafting
- Bone Socket Grafting
- Immediate Implant Placement
- Anterior Implants
Root Canal Therapy-Maxillary 1st Molars
Approximately 85% of all upper 1st molars have 4 canals. The use of the endodontic microscope helps identify the elusive mesial-palatal (MB2) canal. As seen in this case all 4 canals where located, cleaned and shaped and all portals of exit for this tooth were sealed.

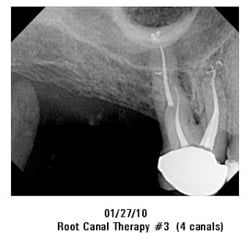
The general dentist requested an adequate post space in the Palatal Root.
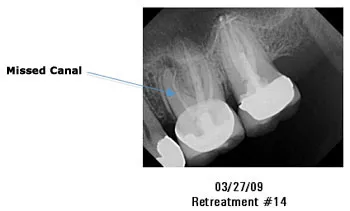
Retreatment Root Canal Therapy
There are times when a previously treated root canal needs to be re-treated. This happens for a variety of reasons. Coronal leakage from the crown, recurrent decay, missed canals, or unusual anatomy are just to name a few. Retreatment
is the ideal treatment in order to thoroughly clean and seal the entire root canal system of the tooth.
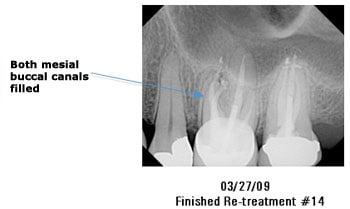
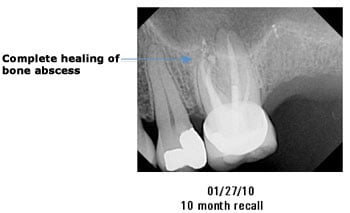
In this case, the maxillary 1st molar was previously treated, however not all the canals where cleaned, shaped and sealed. Therefore the treatment of choice is to retreat the entire root canal system and locate the missing canal since this was the primary reason for the periapical (bone) abscess.
In this case a retreatment was necessary due to recurrent decay under a previous crown. The contamination of the root canal system required a retreatment to be performed along with clinical crown lengthening with a placement of a new post and core.


Apicoectomy (Surgical Root Canal Treatment)
There are times when a previously treated root canal needs to be redone. In some instances, a surgical approach (Apicoectomy)
is the ideal treatment choice.
In this case a large post could have potentially fractured this tooth during a standard re-treatment, therefore an apicoectomy was the decided treatment.

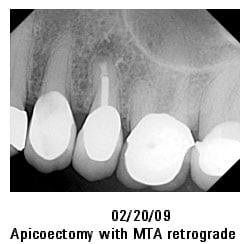
The other situation when an apicoectomy would be the ideal treatment is when a re-treatment is not possible due to an obstruction in the canal. In this case, our patient had a previously treated root canal performed several years ago and now has a recurrent infection. In the mesial root there is an obstruction (separated instrument), preventing a standard re-treatment and therefore an apicoectomy was the ideal treatment of choice in this situation.


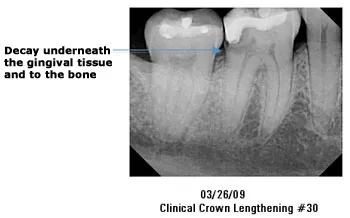
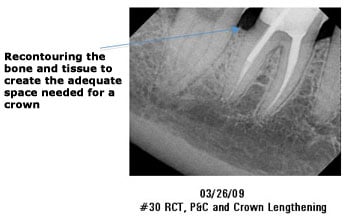
Clinical Crown Lengthening
Clinical crown lengthening is needed when decay on a tooth has extended underneath the gum tissue. In order to remove the decay and have adequate tooth structure to hold a new crown, clinical crown lengthening is needed to be performed.
Intravenous Sedation (IV Sedation)
At times patients need to have IV Sedation in order to have their treatment completed. The primary reasons we treat patients using IV Sedation are:
- Fear and Anxiety
- Inability to get anesthetized numb
- Severe gag reflex
- Medically compromised patients (Ex: Downs Syndrome)
These patients generally have their entire treatment performed at one time due to their special needs.
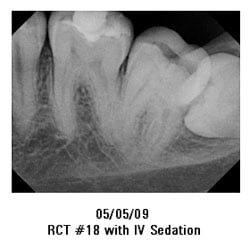
In this case, our patient had a debilitating gag reflex that required him to have his root canal treatment under IV Sedation. What made this case especially important to the patient is that they needed root canals on 2 teeth (#18 and #31), which was performed at one time.



Block Bone Grafting
Whenever a tooth is extracted, and no interventions are planned to preserve the bone, approximately 25-35% of the bone height may be lost within the first year. This can lead to an insufficient height of bone that would be required for an adequate implant to be placed.
Therefore a block bone graft was needed to create the necessary bone height for a future placement of an implant. Platelet Rich Plasma (PRP) was used in conjunction with the block bone graft to help promote and increase a successful grafting of the block bone graft.


Bone Socket Grafting
We are in the practice of trying to save teeth but unfortunately that may not be possible. If endodontic treatment were not an option, then extraction and bone socket grafting would be the preferential choice. The goal is to maintain the most amount of bone possible after a tooth is extraction. That is why we place bone-grafting material after an extraction, along with the use of Platelet Rich Plasma (PRP)
. We have found using PRP with the bone graft maintains the bone level at the most optimal location.
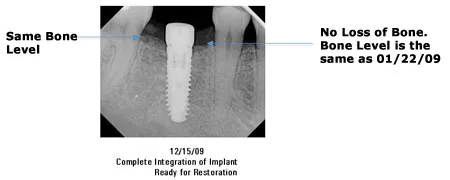
In this case at 6 and 11 months after the tooth was extracted and bone grafted, we see that the level of bone has been maintained at the original level prior to extraction. This allows us to maintain the most amount of bone as possible for an ideal placement of an implant.



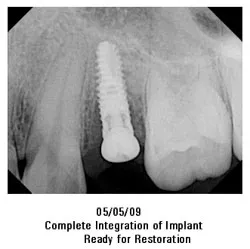
Immediate Implant Placement
There are times when an implant
can be placed immediately after the extraction of the tooth.
This patient was referred for evaluation to see if this tooth was savable. Unfortunately there was an extensive amount of decay and therefore the tooth was determined to be non-restorable.


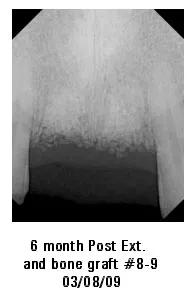
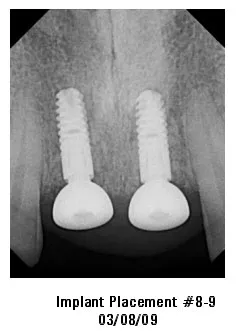
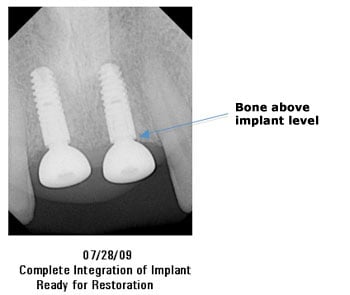
Anterior Implants
Implants in the anterior (front part of the mouth) region can be one of the most complicated implants to place. The primary reason is esthetics. The type of implants can play a large role in creating the most optimal esthetics. The implants that we use allow bone to grow slightly over the implant, thereby minimizing bone loss down to the 1st thread. This allows for the most optimal esthetic outcome.
This patient had non-restorable anterior teeth which we extracted and bone grafted 6 months prior.